
Upper limb amputation can be divided by different amputation levels into finger amputation, hand amputation, forearm amputation, upper arm amputation and scapular belt amputation. Finger and hand amputations preserve as much length as possible and preserve residual finger (end) sensation, hand grip strength, finger grip (thumb, finger) and gripping function. The badly injured thumb should also be preserved and not amputated. In addition, the patient's occupation should be considered to truncate the horizontal plane. In the case of a worker, the metacarpal head corresponding to the second or fifth finger should be preserved during the metacarpophalangeal joint dearticulation to maximize grip strength.
1. Artificial limbs can be fitted on almost any plane.
2. Muscle treatment: traditional - the stump muscles are not sewn together and are conical to fit the plug prosthesis; Modern -- Muscle flaps are required to be sutured, known as myoplasty. The prosthesis is a full contact receiver cavity, which can be fully contacted with the stump, so that the bearing capacity is reasonable, the wear is comfortable, and the stump blood transport is good.
3. Rigid bandage was applied after surgery, and temporary prosthesis was selected immediately or in time to promote the recovery of coordination of both hands.
Indications of upper limb amputation
1. Extensive and severe injuries to limbs that cannot be recovered or preserved and threaten life.
2. Malignant tumors of bone and soft tissue of limbs.
3. Severe infection of the limb (acute infection cannot be controlled; Chronic infection may cause local tissue malignancy.
4. Irreversible limb vascular damage.
5. Irremediable limb deformities.

The choice principle of amputation plane
1. Keep the length of the limb as far as possible -- keep the long arm to make the prosthesis more convenient and powerful.
2. Preserve joints and carpal bones as much as possible -- you can retain some flexion and extension of the wrist joint. Retention of the radioulnar joint - 50% of the pronation and supination function of the forearm can be transferred to the prosthesis. Preservation of the elbow - thus preserving part of the rotation of the humerus, the flexion and extension of the elbow.
3. The humeral head should be preserved as far as possible in high upper limb amputation, so as to preserve the shape of the shoulder and also benefit the stability of the prosthesis.
Principles of treatment of residual tissue
1. The incision
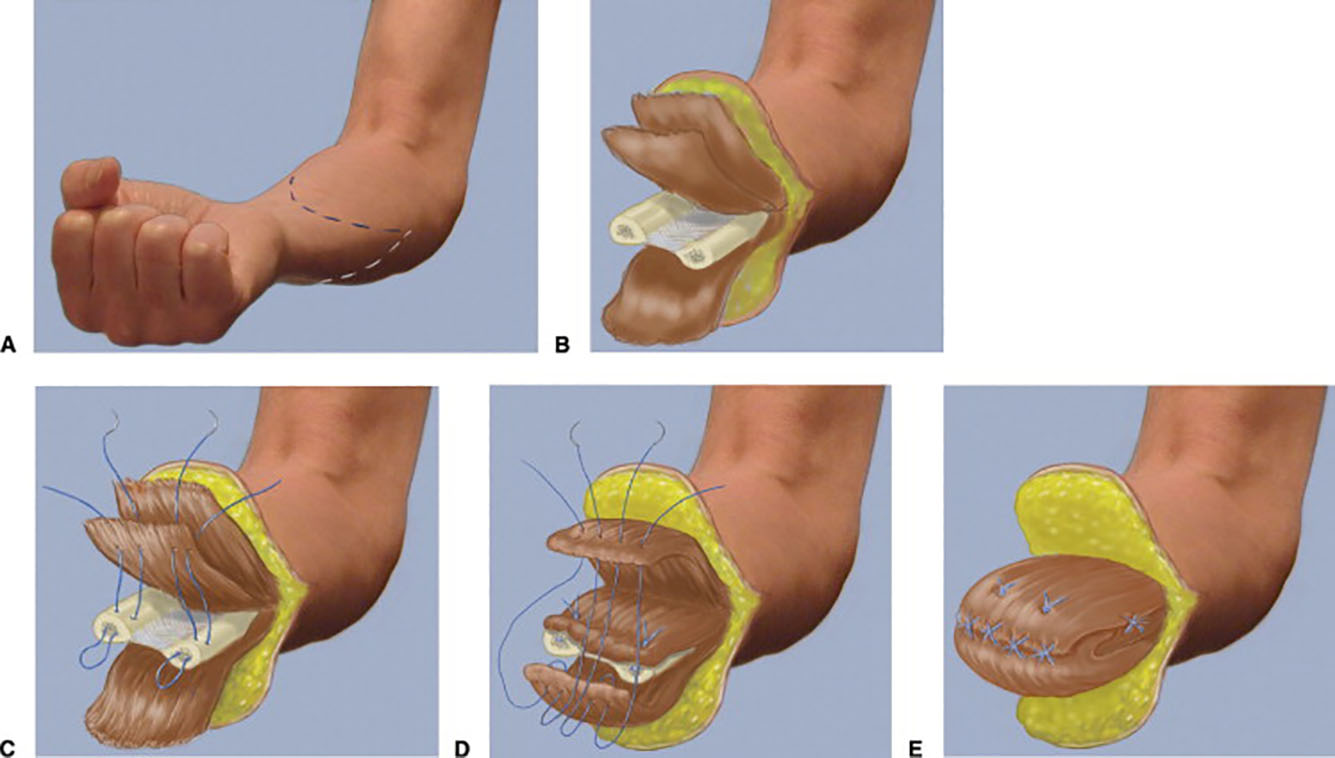
Wrist amputation -- long volar flap, short dorsal flap, length ratio 2:1.
Above the wrist -- anterior and posterior equal length flap, the length is 1/2 of the diameter of the amputation plane.
2. The muscle
The anterior and posterior muscle flaps were sutured opposite to each other and fixed to the bone end if necessary to prevent sliding.
3. Treatment of broken bone ends
The periosteum is cut below the osteotomy level and turned downward to cover the bone tip, sealing the marrow cavity. The synovium of the joint capsule should be completely resected and the articular cartilage scraped down to the subchondral bone.
4. Neural processing
Should not be too much traction, so as to avoid nerve fiber fracture or demyelination changes, postoperative scar, neuroma and stump pain.
5. Vascular treatment
6. Incision suture and drainage
 Thigh Series
Thigh Series
 Lower Leg Series
Lower Leg Series
 Product Video
Product Video
 Group Propaganda Video
Group Propaganda Video



